The Royal London Hospital
Contributed by Survey of London on April 29, 2019
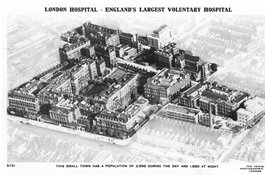
The Royal London Hospital is one of the capital’s largest teaching hospitals,
serving a diverse population of 2.6 million in east London. The institution
was founded in 1740 as the first charitable infirmary on the east side of
London, intended to offer relief to merchant sailors and labourers, and
supported largely by voluntary contributions and donations from its foundation
until the establishment of the National Health Service (NHS) in 1948. The
hospital has been an important landmark on the south side of Whitechapel Road
since it transferred to this site in 1757, when it was surrounded by open
fields. Over the next 250 years the hospital expanded gradually to become a
sprawling healthcare complex, due to local population growth and advances in
medicine and surgery. Its piecemeal evolution was also a reflection of
uncertain finances and fundraising efforts. From the late nineteenth century,
the hospital spilled into purpose-built detached specialized blocks and a
cluster of nurses’ homes was constructed in its immediate vicinity. The
footprint of the hospital has recently contracted for the first time in its
history, with its transferral to a modern tower block to the south of its
historic base. Overlooked by its towering successor, the retained former
hospital is set to be refurbished and extended to provide a new civic centre
for Tower Hamlets Council. Along with its long and continuing significance to
the public life of the area, the Royal London Hospital is celebrated for its
association with brilliant minds and significant individuals, such as the
pioneering surgeon Henry Souttar and the heroic nurse Edith Cavell. A darker
fascination endures around the hospital’s faint connection with Jack the
Ripper and its provision of a permanent and compassionate home for Joseph
Merrick, known popularly as ‘the Elephant Man’.
Early History, 1740–1778
Contributed by Survey of London on April 29, 2019
Foundation
The Royal London Hospital traces its beginnings to September 1740, when seven
men met at a tavern in Cheapside to consider plans for establishing a new
infirmary. Shute Adams, druggist, Josiah Cole, apothecary, John Harrison,
surgeon, and Richard Sclater, were affiliated with the medical profession,
while Fotherley Baker, lawyer, John Snee, girdler, and George Potter were
associated with commerce and the law. At its inception, the hospital joined a
rich thread of charitable infirmaries in the capital, including St Thomas’s
and Guy’s in Southwark, St Bartholomew’s and Bethlehem in the City, and St
George’s at Hyde Park Corner. Its founders possessed a common concern for the
care of labourers and merchant seamen, along with their wives and children.
There was not yet a hospital to serve the east of London and its rapidly
growing population, mostly dependent on employment in industry and trade
connected with factories, sugar refineries and the port. A fund was raised to
establish a new hospital that would offer assistance without charge to its
patients. At the first official meeting of the founders, Harrison presented a
five-year lease of a house in Featherstone Street, Moorgate, taken for the new
infirmary. A motion to establish the charity met with unanimous approval. No
time was wasted in acting upon this resolution and in November 1740 the
hospital opened its doors to patients as the London Infirmary. The charity
received patients sent by its governors, as well as people who arrived without
a recommendation. The house contained about thirty beds for inpatients and
cases were also taken as outpatients, but incurables were not admitted.
Harrison, Cole and Dr John Andree, a physician who had trained in Reims,
attended on a daily basis without pay as surgeon, apothecary and physician.
These honorary posts were supported by salaried staff, including a matron, a
porter, nurses, and night watches.
Within six months of its foundation, plans were afoot for the infirmary to
‘take a larger house in a more convenient situation’. By April 1741, a
house was secured on the south side of Prescot Street, Goodman’s Fields. This
location was judged to better serve the charitable interests of the hospital
due to its proximity to the dwellings of both Spitalfields labourers (who were
overwhelmingly weavers) and merchant sailors near the Thames, and its distance
from any other hospital. A lease of the house was agreed for a term of just 3½
years. The infirmary moved the following month and opened with room for about
forty beds. A shop was also purchased in nearby Alie Street for an
apothecary’s store and, in 1742, another house was taken on Prescot Street to
isolate patients with venereal disease.
Need for enlargement
By 1743, the expiration of the lease was looming and its renewal under
consideration. Plans for the provision of a new building for the hospital were
sparked by the intervention of Isaac Maddox, Bishop of Worcester, who was
invited to deliver a sermon at the charity’s annual anniversary feast in April
1744. The matter of the lease was still unresolved and uncertainty surrounding
the hospital’s future in Prescot Street probably struck a chord with the
bishop’s philanthropic interests. From modest origins as an orphan, Maddox
rose to become a prominent and charismatic voice in support of charitable
hospitals, including the St Pancras Smallpox Hospital and Worcester County
Infirmary. He is commemorated by a funerary monument in Worcester Cathedral
which bears a depiction of the Good Samaritan and an epitaph that remembers
him as an ‘Institutor of Infirmaries’. In his sermon, the bishop argued
that the infirmary was overcrowded and inadequate: ‘admittance is impossible;
the scanty building waits your necessary assistance to enlarge its
bounds’. This declaration spurred the charity into action; a donation of
twenty pounds from the bishop was allocated for the enlargement of the
hospital and a fund opened for a new building.
An agreement with Richard Alie, landlord at Prescot Street, satisfied the
immediate need for enlargement. The house was re-taken on a lease of twenty-
one years from Christmas 1744, along with three adjoining houses and a shed at
the end of the garden. An extensive programme of repairs and improvements
followed which, by 1745, had reached such an intensity that the supervision of
a surveyor was required. Isaac Ware was appointed to this honorary role in
return for compensation of his travel expenses. Ware was in a secure position
to perform the duties of hospital surveyor, having been the architect of the
conversion of Lanesborough House at Hyde Park Corner into St George’s
Hospital.
An inspection of the houses by a committee of governors, including surgeon
Harrison, initiated plans to repair or rebuild the shed. It became apparent
that it was too dilapidated for renovation and that a new building was
required to accommodate a range of functions, including a waiting room, a
chapel, a laundry, a distillery, a laboratory, a mortuary, and a cold bath.
Ware was instructed to prepare designs and Joel Johnson and Robert Taylor were
contracted as builders in partnership. The building was completed in 1747, yet
the House Committee was troubled by reports that the cold bath was poorly
finished and complaints from neighbouring residents about a cesspool emptying
into Chamber Street. By June, Ware judged it ‘impossible’ to continue as
surveyor due to ‘the distance of his abode, and the multiplicity of his other
business’. James Steer was invited to take his place. The committee may
have hoped to benefit from Steer’s experience as surveyor at Guy’s Hospital,
where he designed its east wing in 1738–9. Yet Steer’s involvement was
fleeting: like his predecessor, he was distracted from his honorary post by
fee-paying ‘business’. Boulton Mainwaring, surveyor and son of a Staffordshire
surgeon, was then invited to assess the cold bath and sanitary arrangements
and by August 1747 was acting as surveyor. This was the beginning of a long
tenure as hospital surveyor; Mainwaring was to play a pivotal role in securing
the site for a new building on Whitechapel Road and designing the hospital’s
first purpose-built home.
Search for a site
Consideration of the need to secure a permanent home for the hospital
continued after the building works of 1746–7. While these measures had
improved conditions at the infirmary, they did not guarantee a long-term
solution to the problem of overcrowding. The refusal of a lease extension
struck a fatal blow to any plans to remain at Prescot Street. In June 1746,
Richard Leman (formerly known as Alie), confined to his country estate with
gout, had declined to grant an additional term. This outlook, coupled with
concern that the houses would be ‘too old and ruinous to continue in longer’,
prompted the House Committee to revisit the Bishop of Worcester’s campaign for
a new building. In December 1747 a committee of governors was appointed
to secure a suitable piece of ground on the east side of London, close enough
to the City for the convenience of its governors, physicians and
surgeons.
The sub-committee was ordered to proceed in its search with ‘great management,
secrecy and expedition’. They had not met with any success by April 1748,
and the task of finding a site was delegated to Mainwaring. In June, he
reported that the only suitable site was that ‘commonly known by the Name of
White Chappel Mount and the Mount Field’. Situated on the south side of
Whitechapel Road, an arterial road which offered a direct route to and from
the City, the largely open site was well-positioned to answer the charitable
aims of the hospital, being near to the workplaces and dwellings of its
nominal patients and at a distance from any other hospital. It was in the
possession of Samuel Worrall, most likely the carpenter and builder prominent
in development in Spitalfields between 1720 and 1750. He offered to part with
his interest in the land in Whitechapel, which he held on a sixty-one-year
lease from the City, for £750. Mainwaring intended offering about £600 and
thought a longer term could be obtained easily as the City held the land from
the Wentworth estate for a term of 500 years. Worrall insisted that his high
price would only cover the expense already incurred of some new buildings on
the land.
The hospital began negotiations with Worrall, specifying an interest in the
undeveloped land. In October 1748, newspaper reports stated that the hospital
had taken a piece of ground and was proceeding to erect a building, when the
matter was actually far from settled. The hospital was still in negotiations
with Worrall, and considering other properties. These included sites in Lower
East Smithfield, Leadenhall Street, Houndsditch and Bethnal Green, along with
the adaptation of London House in Aldersgate Street. Greater consideration was
given to two other sites in Whitechapel, yet one was too expensive and the
other objectionably close to a white-lead works. In August 1749, the situation
was still uncertain and Worrall now offered his land for the higher price of
£800, which was received as ‘very improper’. William Myre, a governor, was
asked to make an appeal to his acquaintance Lucy Alie for the hospital to
purchase the freehold of its premises at Prescot Street. This tactical
change may be ascribed to a hope that their new landlady, who had recently
inherited Leman’s estate, might be more amenable. Yet the scheme led nowhere
and by October the committee had returned to Worrall, who now offered a £40
deduction and asked for his son to be made a life governor of the charity to
compensate for his expenditure on improving the land. In December the hospital
reached an agreement with Worrall to purchase the land for £800, with the
condition that the City would grant the hospital its long-term copyhold.
Negotiations with the City Lands Committee for its 500-year lease from the
Wentworth Estate were no less intricate. As the hospital was not an
incorporated body, the City could not make an agreement with the charity but
was prepared to make a deal with six or more gentlemen acting on its behalf.
The City also indicated that it was only willing to part with the field lying
east of Whitechapel Mount. Richard Coope, George Garrett, Dr James Hibbins,
Boulton Mainwaring and Richard Sclater offered to act on behalf of the
hospital. By July 1750, they had agreed to acquire the City’s interest in the
Mount Field for the remainder of its 500-year lease.
Mainwaring’s design
In May 1751, the hospital’s building committee instructed Mainwaring to
prepare a plan for a building to accommodate 200 patients, with provision for
future enlargement. He presented five plans to the building committee, of
which two were selected for further consideration. No drawings of the five
designs survive but the minute books record that one of the selected plans was
designed to accommodate 198 patients in each wing with a total capacity of
396, whereas the other would accommodate 366 patients.Mainwaring was
instructed to seek advice from the hospital’s physicians and surgeons,
particularly in relation to room height, and to prepare estimates. The
committee decided that the projected expense of both plans was excessive and
that a smaller building ‘might be sufficient for the present’. Mainwaring
was asked to draw up a new plan ‘as near as he could’ to one of the proposals
for a hospital for 300 patients that could be extended as required in the
future, along with estimates for the building with, and without, ornament.
Revised designs for a building for 312 patients were presented to the
committee in September and ‘plan and elevation number six without the
ornaments’ approved.
The chosen design was for a hospital composed of three detached ranges linked
by colonnades. No drawings of this early plan survive, but a description of
its basic form recalls Wren’s unexecuted designs for Greenwich Hospital of
1694–1700 and Gibbs’s plan of around 1730 for the rebuilding of St
Bartholomew’s. Mainwaring might also have borrowed from the Foundling
Hospital, built between 1742 and 1754 to designs by Theodore Jacobsen. The
main hospital buildings there were planned as three detached ranges linked by
short lobbies, enclosing three sides of a courtyard.
Whatever the projected advantages of the chosen plan, by the next month it had
been reconsidered ‘under the several heads of accommodation, convenience,
durableness, and expense’, and declared ‘capable of great improvements’.
Mainwaring, whose efforts had moved to examining the site in preparation for
foundations, prepared a new design for a single building with attached
wings. This was considered superior on each of the four points. Firstly,
it would accommodate 350 patients. Secondly, its arrangement was judged to be
more convenient for patients and staff, with south-facing wards (deemed the
preferable aspect for patients) and protection from weather conditions and
dust from Whitechapel Road. Thirdly, the committee argued that a continuous
building would be ‘in its nature stronger and more lasting, than the same
quantity divided into three’. Finally, the plan for a smaller building was
less costly and saved the expense of colonnades. In another economising
measure, plans for a chapel were omitted as prayers could held in the court
room. It was also decided that the hospital should be positioned parallel to
Whitechapel Road and set back by seventy feet or more for the governors’
coaches. In December, Plan No. 8 was approved by a General Quarterly Court and
Mainwaring appointed as surveyor for the proposed building.
The final plan was publicized by an engraving produced by John Tinney, who was
commissioned to carry out the work with ‘all expedition’. Three hundred copies
were circulated to the governors to generate donations to the building fund,
and also to reassure benefactors that there was ‘nothing ostentatious,
sumptuous or unnecessary intended’ in its design. Mainwaring’s final
design for the new hospital reflects this concern for avoiding extravagance.
The north front was to have a plain, symmetrical façade of twenty-three bays
with a projecting centre capped with a pediment. With ornament on the exterior
restricted to a Doric entrance porch, a dentil cornice and stone doorcases at
the side entrances, the main elevation was modest yet dignified in character.
The new building had a U-shaped plan composed of a three-storey central block
with two rear wings, east and west. The main block contained a central
corridor and two large wards positioned on the south side of each floor. The
wards were serviced by lobbies containing sinks, privies, and nurses’ rooms.
On the ground floor, the north side of the central block was occupied by
offices for the apothecary, physicians, nurses and stewards. The first floor
had a large court room that doubled as a chapel at its centre, flanked by
offices for the surgeon, matron and secretary. The rear wings, identical in
plan, contained back-to-back wards separated by spine walls with central
fireplaces; an arrangement similar to the ward blocks at St Bartholomew’s.
Construction
The hospital was constructed to Mainwaring’s plain and practical design
between 1752 and 1778. The central block was built first and completed in 1759
under his supervision. The east wing was built in 1771–4 and the west wing in
1773–8, both under the supervision of Edward Hawkins, who succeeded Mainwaring
as hospital surveyor in 1771.
Central block, 1752–9
After plans for the new building were settled in December 1751, Mainwaring’s
efforts turned to its construction. John Mann, carpenter, and Thomas Andrews,
bricklayer, were contracted to build up to first-floor level. The foundation
stone was laid on 11 June 1752 in a ceremony attended by noble patrons and
dignitaries. Progress was swift, yet it seems that the building committee felt
that it would be too risky to attempt the entire building. When the workmen
completed their contracts in December, Mainwaring was asked to prepare
separate estimates for finishing the central block and its wings. In February
1753, new contracts were advertised for completing only the central block. Yet
before any were agreed, Mainwaring’s report on the cost of finishing the
central block delivered a blow to the building committee. His estimate of
£5,300 was far higher than the sum of cash held in the building fund and
annuities held in the name of trustees, leaving a shortfall of more than
£1,150. Despite the shortage of funds, building works stumbled along. In April
and May, Edward Gray was hired as bricklayer, Joseph Clark as carpenter and
Sanders Oliver as mason. Progress remained steady, suffering only occasional
setbacks. The only serious and recurring obstacle was cash flow. Mainwaring
increased his estimate for the central block to £5,700, and, though it was
covered in by the end of March 1754, work then came to a halt due to a lack of
funds. The suspension of building activity coincided with worsening
conditions at Prescot Street. The hospital’s governors convened to consider
the situation and emphasized the importance of finishing the new building. A
subscription was launched to raise funds and the building committee ‘readily
agreed’ to an offer from several governors to lay one of the floors at their
own expense. Donations trickled into the building fund and work resumed
in 1755, when workmen were employed to finish the new building. Gray and
Oliver continued as bricklayer and mason, and Joel Johnson was appointed as
carpenter and joiner, despite the debacle over shoddy workmanship at Prescot
Street. Building works now progressed steadily without any serious hiccups
and, though they continued until 1759, the hospital moved into its new
building in Autumn 1757. The lease of the infirmary’s houses on Prescot Street
was relinquished immediately.
The allocation of rooms in the completed range did not differ from
Mainwaring’s final design. The cellar storey comprised a long passage
providing access to stores, laundries and wash-houses paved with Purbeck
stone. The south-facing wards of the central block had large stone
chimneypieces and were furnished with plain wooden bedsteads. A handful of
rooms, including the court room, the committee room and offices for the
physician, surgeon and apothecary had wainscoting to a height of five feet. A
surgery, a bleeding room and a cold bath were positioned on the ground floor,
and an operating theatre in the attic. The central block successfully brought
together all of the hospital’s activities under a single roof, with room at
first for 130 patients. The number of beds increased in the following years
and by 1765, there were 190.
East wing and west wing, 1771–8
After the completion of the central block, plans to build the proposed side
wings rested until 1770. The revival of building activity coincided with
improved finances, bolstered by a legacy from Anne Crayle, a spinster
landowner who bequeathed much of her wealth to the capital’s voluntary
hospitals. Despite this significant boon, the newly reinstated building
committee proceeded cautiously. At first Mainwaring was asked to prepare a
plan and an estimate for a single wing, to be constructed on the foundations
already laid. His plan for the east wing conformed to the original design for
identical three-storey wings of six bays, with paired wards on each floor and
a basement. In 1771, Thomas Langley was appointed as carpenter, Thomas Barnes
as bricklayer, and Isaac Ashton as mason. As work on the east wing commenced,
Mainwaring warned that he was struggling to perform his duties, particularly
‘the constant attendance upon the workmen requisite’, due to the distance from
his home. He recommended that Edward Hawkins, a local developer on the Leman
Estate in Goodman’s Fields, should act as surveyor in his absence, yet
promised to attend as frequently as possible. However, poor health
intervened and at the end of the year, at the age of sixty-nine, Mainwaring
resigned.
Under Hawkins the building works progressed steadily. Contracts were agreed to
finish the east wing in 1772 and by the following spring, its completion was
in sight as advertisements were circulated for a contractor to furnish it with
ninety beds. At this point, there was enough optimism for the hospital to
assemble a building committee to manage the construction of the west wing;
that took place in 1774–8 and included many of the same workmen.This ambitious
strategy soon faltered under financial pressure. An appeal for donations in
1774 revealed that the completion of the east wing and shell of the west wing
had depleted the building fund, leaving a shortfall of cash to pay the workmen
and a deficiency of almost £900 to finish the building. Despite these
financial straits, work trundled forward. A plea for support was successful by
the following year, when the building committee reported that its fund
contained over £1,000 for finishing the west wing. This news prompted a flurry
of activity and by December 1777, the west wing was largely finished.
The completion of the west wing in 1778 signified the realisation of
Mainwaring’s design for the hospital’s first purpose-built home. At this point
in its history, the hospital overlooked Whitechapel Road from its position
east of the Mount and was bounded by open fields to the south. By the mid
1780s, a narrow range had been added at the west end of the hospital to
provide coach houses and a mortuary. Improvements were also made to the
hospital’s immediate surroundings: a patients’ garden was nestled between the
ward wings and a kitchen garden cultivated from waste ground at the west. The
charity, by now known as the London Hospital, released pamphlets which boasted
of its convenient location close to the shipping activities of the port and
Spitalfields, a nucleus for manufacturing, as well as the health benefits of
its ‘airy situation’. With eighteen wards fitted up with about 215 beds, the
new building offered a permanent base from which the charity could intensify
its work. By 1786, the charity had treated nearly 450,000 patients since its
modest beginnings, cementing its status as an institution of critical value to
impoverished working families in the east of London.
West wing and east wing extensions, 1830–42
Contributed by Survey of London on April 29, 2019
Plans for the first substantial enlargement to the hospital arose in 1830 in
response to rising patient numbers, a by-product of rapid population growth.
The establishment of the enclosed docks and the expansion of local
manufacturing demanded an army of labourers. Many ended up residing in densely
populated slums prone to the spread of disease, and were exposed to ‘fearful
and appalling accidents’ at work. A newly assembled building committee
observed that within a year, the hospital had been forced to refuse admission
to more than 870 cases. A wing extension promised to provide ninety additional
beds and separate wards to isolate contagious patients. These motivations
coincided with low construction costs and a significant legacy from Edward
Hollond, a governor with property in Cavendish Square and Suffolk. The
committee anticipated that an extension to one of the rear wings would cost
£8,000, which would be covered securely by Hollond’s bequest, existing funds
and a fundraising campaign.
Alfred Richardson Mason, hospital surveyor since 1821, was asked to prepare
plans for a wing extension. His father, William Mason, was a local bricklayer
and governor who had applied unsuccessfully for the post of surveyor during
its last vacancy in 1806 and served on the hospital’s building committee. The
chosen plan was reviewed by the medical staff and many of their
recommendations adopted. Mason proposed extensions to the east and west wings
to provide new wards. The external appearance of the extensions matched the
austerity of Mainwaring’s design. On each side a three-bay projection, capped
with a pediment, connected the existing wing to a new ward wing composed of
six more bays. On the ground, first and second floors, Mason’s plan followed
the arrangement of paired wards separated by a spine wall with a central
fireplace. The new wards were connected to the earlier wards by lobbies, each
containing a washing room and a bath room, along with a kitchen and a nurses’
room. In the basement of the west wing, the extension was allocated to the
hospital’s medical officers: a long patients’ waiting hall was bordered by a
dispensary and separate physicians’ consulting rooms. Staircases in the
second-floor lobbies rose to an attic storey with rooms for special cases,
including separate rooms for private patients in the east wing and a ward for
contagious cases in the west wing. The hospital was surrounded by an
assortment of open spaces, including a drying ground adjacent to the laundry
and a burial ground to the south of the quadrangle.
William Colebatch was employed as contractor for the west wing extension in
June 1830, and construction began without delay. The new wards opened in
August 1831 and were fitted up with fifty iron bedsteads, an improvement from
the earlier wooden beds judged to be ‘receptacles for and filled with
vermin’. Although the number of beds was considerably less than the
ninety initially intended, the extension proved to be of immediate value as it
opened before the first outbreak of a cholera epidemic. Sir William Blizard,
eminent surgeon to the hospital, circulated a plea to the House Committee for
special procedures to combat its spread, including the provision of an
isolated place to receive sufferers. Although the hospital declined to admit
cases of cholera, on the grounds that it was an untreatable disease, the new
attic ward was used to isolate infected inpatients.
A lack of funds delayed the construction of the east wing extension, as the
hospital struggled with financial pressure caused by rising patient numbers.
An appeal for donations launched during the charity’s centenary year was a
success. Robert and George Webb were contracted as builders in December 1840.
The extension was finished in 1842 and Mason paid a fee equal to five per cent
of the building costs; by now the position was no longer honorary and this was
termed the ‘usual’ surveyor’s commission. The only significant departure
from Mason’s earlier plan wasthe provision of separate wards for Jewish
patients, which arose from a request delivered in 1837 by a committee of
Jewish gentlemen devoted to ‘the more effectual relief of the sick poor of the
Jewish community requiring medical aid in and about London’. This deputation
on behalf of ‘Gentlemen of the Hebrew Nation’, noted for their generosity and
support towards the hospital since its inception, was made by Joel Emanuel and
Abraham Levy. In addition to exclusive wards for Jewish patients, the
committee requested a team of Jewish medical staff and a separate kitchen to
prepare kosher food. By these measures, it was hoped that Jewish patients
would ‘receive that consolation and peace of mind which would prove most
consonant with their religious feelings’. Although the committee offered
some financial support and predicted the initiative would encourage donations,
the project was deferred until funds were secured for the hospital’s
enlargement. The centenary festival attracted donations and, when the east
wing extension was completed, two wards in the earlier part of the hospital
were set aside for men and women.
The effects of this improvement were not permanent due to demand for beds. By
1854 the House Committee had decided to allocate portions of wards to Jewish
patients as an interim solution until a future enlargement of the hospital.
Despite this failure, the wing extensions were considered an overall success.
Their completion was followed by a sharp decline in mortality rates inside the
hospital from ten per cent to eight per cent, and then as low as six per cent.
Further alterations to the east and west wings followed in 1853–4, with the
addition of fireproof staircases and water closets at the south ends to
designs by Mason. This extension was carried out by George Myers, along with
the formation of staff dormitories in the attics of the north end of each
wing.
Alexandra Wing, 1864–6
Contributed by Survey of London on April 29, 2019
Over time, the hospital was increasingly inundated with patients arriving from
the local area and remoter parishes such as West Ham. Since the completion of
the wing extensions of 1830–42, the volume of patients had more than doubled.
By the 1860s, more than 30,000 people were treated as inpatients and
outpatients each year. Overcrowding was not confined to the wards, as medical
officers and nurses endured cramped conditions with little promise of rest.
Due to prolonged shifts and a lack of dormitories, nurses were frequently seen
to be ‘overcome with sleep’ and the matron insisted that her staff could not
be increased without additional sleeping accommodation. By 1862 the situation
had become untenable and a report on overcrowding pronounced ‘a very serious
defect in the arrangements of the London Hospital’.
The hospital turned to its surveyor, Charles Barry Jr, to prepare plans for an
extension to the outpatients’ department. Acting as hospital surveyor from
1858, Barry approached his responsibilities in an efficient manner from
offices in Sackville Street, proposing to attend committee meetings for an
extra charge in addition to a nominal salary and commission rate. Barry
designed a long single-storey building that would run parallel to the existing
surgical and physicians’ outpatients’ departments housed in the west wing. Yet
plans for this extension were stalled as the House Committee contemplated a
solution for the longer term. The matter was delegated to a building
committee, which promoted substantial alterations and argued that ‘the entire
system is one of undue pressure, subversive of sanitary arrangements,
inconvenient to the professional staff, (and) unfair towards the patients and
the servants of the hospital’.
The proposed solution was to build a three-storey wing with a basement and an
attic, extending west parallel to Whitechapel Road. Barry’s plan promised room
for about seventy beds, with separate wards allocated for children, obstetric
cases, and Jewish patients. The hospital had received a series of requests for
the reinstatement of separate Jewish wards since their closure, but was
limited by the pressure on hospital spaces. The wing extension enabled the
hospital to arrange Jewish patients in separate wards on one floor, near to a
kosher kitchen. The new wing was divided roughly into two parts. A three-
storey maisonette with bedrooms and servants’ quarters was carved from the
west end of the wing for the house governor, a resident officer who managed
the daily workings of the hospital and its expenditure. Each floor of the east
side of the building comprised a central corridor flanked by wards or offices.
The basement secured a new surgical outpatients’ department, with an extensive
waiting hall to make the customary ‘lengthened detention’ less onerous, and a
consulting room flanked by rooms for dressing injuries. An attic dormitory for
night nurses addressed fears that a lack of supervision compromised their
efficiency and ‘quality’. The intermediate floors were given over to wards,
with the exception of a new committee room and secretary’s office positioned
on the ground floor.
The exterior of the west wing reflected its disjointed plan. On the north
elevation facing Whitechapel Road, a projecting bay capped with a pediment
marked the junction between the wards and the house governor’s residence. The
west elevation had a raised entrance porch to the house governor’s maisonette,
which overlooked a private walled garden at the south. A significant
innovation in the new wing was the construction of a narrow tower to contain
sanitary facilities, specifically a water tank at its peak and water closets
below. At Barry’s insistence, the building was constructed with fireproof
concrete floors and staircases. The House Committee initially hesitated over
the additional expense, yet was persuaded by the surveyor’s warnings that the
hospital could be criticized for failing to introduce fireproof floors, which
also possessed soundproof and ‘verminproof’ qualities.
The new wing was constructed in 1864–6 by Hill & Keddell, contractors
based in Whitechapel Road. It was financed partly by charitable donations,
including substantial gifts from local businesses and the brewer Sir Thomas
Fowell Buxton, chairman of the House Committee. Many of the hospital’s staff
and supporters were recognized in the naming of the wards: one was named
‘Buxton’, and ‘Davis’ commemorated the present and former vice-presidents. A
ward was named ‘Blizard’ in memory of the hospital’s eminent surgeon. The
foundation stone was laid in July 1864 in a ceremony that saw Whitechapel
awash with crowds and decorated with bunting. The building was bestowed with
the first name of the new bride of the Prince of Wales, an association
intended to inspire ‘respectful admiration’. Its opening was not
accompanied by such celebration; formal inauguration had to be abandoned due
to another outbreak of cholera. In July 1866, patients were moved into the new
wing to provide space for cholera patients.
The completion of the Alexandra Wing allowed various improvements to be
effected elsewhere in the hospital, as rooms were modified and reassigned.
These alterations were also carried out by Hill & Keddell and continued
until 1868. In the basement, an ophthalmic ward was set up and the medical
outpatients’ department extended into rooms formerly occupied by its surgical
counterpart. On the ground floor, the entrance vestibule was extended and a
large receiving room added at its west. Bedrooms, sitting rooms and offices
were provided to improve conditions for the medical officers and their
pupils.
Rowland Plumbe and Joseph George Oatley oversaw various alterations to the
Alexandra Wing in the twentieth century, including the formation of a
coroner’s court in the basement and a single-storey extension at the west. An
endowment by James Hora, a vice-president of the hospital, led to the opening
of the Marie Celeste maternity department in 1905. Due to persistent pressure
on vacant space for hospital expansion, the house governor’s private garden
was not destined to survive. By 1960 it had been converted into an ambulance
station, with a covered parking bay and ramped entrance into the hospital.
This in turn was short-lived, as the Alexandra Wing and the adjoining
ambulance station were cleared for redevelopment in 1974.
Grocers’ Company’s Wing and further expansion, 1873–6
Contributed by Survey of London on April 29, 2019
The hospital expanded eastwards in 1873–6 with the construction of the
Grocers’ Company’s Wing, a post mortem department and a nurses’ home. Their
completion secured the London Hospital’s status as one the largest general
hospitals in the country, with almost 800 beds. The only surviving remnant of
this building programme is the north range of the Grocers’ Company’s Wing,
which presents an orderly 120ft frontage to Whitechapel Road terminating at
its junction with East Mount Street. Two bays of the south part of the wing
survive in 2019; the rest was cleared in the 1960s for the construction of the
Holland Wing.
This significant enlargement was catalysed by rising numbers of inpatients.
Despite the completion of the Alexandra Wing in 1866, the hospital struggled
to keep pace with the demand for beds. In 1870 the house governor, William
Nixon, recorded an ‘extreme pressure of inpatients’, exceeding 500 at any one
time. Parts of the old medical college were converted into quarantine
wards for contagious cases and wards for patients afflicted with erysipelas, a
bacterial skin infection, opened in a single-storey building in East Mount
Street. The provision of isolation wards evidently failed to secure a long-
term solution to overcrowding. A few years later, Nixon reported an alarming
‘state of repletion’ in the wards. He declared that the hospital was ‘not
large enough’ to fulfil the demands of the surrounding district, despite its
strict policy of admitting only urgent and curable cases. This deficiency
was exacerbated by the practice of providing separate accommodation for more
than twenty-one types of inpatients, for the most part divided by gender,
treatment, and medical condition. This classification system led to frequent
shortages in beds for particular cases, which made it necessary to mix
different types of patients in the wards. Additional room was most urgently
required for medical cases, children and obstetric patients.
The proposed solution was to extend the hospital to provide 200 additional
beds, increasing the number of inpatients by a third. A public fundraising
campaign was launched with the aim of securing £100,000 towards the
construction and operating costs of an enlarged hospital. A new wing extending
east from the central block was deemed preferable to ensure the proximity of
wards to the ‘working centres’ of the hospital, namely the lifts, the staff
offices, the laundry, the kitchen, the operating theatre, and the
depository. The intended site was occupied by the old medical college and
a carriage shed fronting Whitechapel Road, along with various workshops, sheds
and stables in East Mount Street. The building programme was overseen by
Charles Barry Jr, who had assumed the position of consulting architect to the
hospital in 1870. The House Committee had reorganized Barry’s responsibilities
amid concerns that he was ‘too much engaged in other directions to give
sufficient personal attention to his duties’. He was invited to adopt an
advisory role and to delegate supervision of repairs to a salaried surveyor.
This task was assigned to J. A. Thornhill, the clerk of works during the
construction of the Alexandra Wing.
The centrepiece of this wave of hospital expansion was the Grocers’ Company’s
Wing, named in recognition of a donation from the City livery company. Their
gift was accompanied by various conditions, including that the wing should be
completed within three years. While the House Committee had intended to
postpone building work until the fundraising campaign had realized its target,
the Company stipulated that construction should begin immediately. As the
projected expense of the wing exceeded £25,000, it was reasoned that sole
responsibility for its design should be entrusted to Barry. He planned a
three-storey wing with a basement and attics, with an L-shaped plan composed
of two blocks; a north range extending east from the front block in line with
Whitechapel Road, and a south range running along East Mount Street. This
arrangement preserved a yard between the extension and the main building, with
the benefit of supplying light and ventilation to the inward-facing wards. The
principal floors followed the pattern of the earlier ward wings in plan,
comprising paired back-to-back wards separated by a central spine wall with
fireplaces. Partitions at the west end of the wards formed linen stores and
areas for water closets, kitchens and sinks. The attics provided dormitories
for seventy nurses.
The foundation stone was laid on 27 June 1874. Construction by Perry & Co.
was complicated by the intended route of the East London Railway, set to curve
beneath the north-east corner of the wing. As a precautionary measure, the
foundations nearest the railway line were excavated to a depth of thirty-five
feet and filled with concrete. The outward appearance of the wing matched the
austerity of the Alexandra Wing, with plain brick elevations decorated by a
string course and a dentil cornice of Portland stone. Its tiled roof was
punctuated by pedimented dormer windows and tall brick chimneys with
oversailing tops. Two rear sanitary towers rose above the roofline of the wing
with louvred openings and steeply pitched roofs; one contained a water tank
and the other was fitted with a ventilation shaft. There were fireproof
floors. At street level, a wooden carriage shed built in 1876 occupied the
narrow stretch between the north front and Whitechapel Road.
The Grocers’ Company’s Wing was formally opened by Queen Victoria in March
1876, in a celebration reported to have lent ‘an attractive and joyous aspect
to (an) ordinarily dull and dingy but busy quarter’. In the following
months, patients were moved gradually into the new wards, which were praised
for their ‘light and pleasant aspect’. The wards were fitted with
specialized ventilation systems devised by Thomas Elsley and George Jennings.
Two rows of evenly spaced beds extended across the long walls of each ward.
This utilitarian arrangement was relieved by potted flowers and pictures on
the walls, and formal plaques bearing the name of each ward. At the time of
writing (2019), the appearance and plan of the north range of the Grocers’
Company’s Wing had survived with only minor alterations, despite adaptation
and changes in room use.
The scale and siting of the Grocers’ Company’s Wing precipitated improvements
elsewhere in the hospital. The new wing was preceded by the reconstruction of
the post mortem and pathological departments in 1873–4. These departments were
formerly housed in the old medical college, and set to be displaced by its
demolition (see below). Their new base was a single-storey building in East
Mount Street. As no drawings survive, little is known about the form of the
post mortem department aside from its provision of a pathological room and a
post mortem theatre. The building was constructed by Perry & Co. to
Barry’s design. Plans for the new wing also gave rise to a scheme for the
hospital’s first purpose-built nurses’ home.
Remodelling and enlargement, 1890 to 1905
Contributed by Survey of London on April 29, 2019
Between 1890 and 1906, every part of the hospital was extended, rebuilt or
remodelled under the supervision of the architect Rowland Plumbe. This
ambitious building programme upgraded the hospital in line with shifting
ideas, innovations and specialization in healthcare. The use of anaesthetics
from the 1840s had extended surgical practice, contributing to an increase in
the number of operations carried out in general hospitals. This pattern was
reflected at the London Hospital, where 420 operations were performed in 1881,
1,114 in 1891, and 2,711 in 1901. New operating suites were designed with
separate anaesthetic rooms to relieve patients from entering theatre in a
conscious state. Ventilation was an established planning concern in hospitals
due to the miasma theory, which held that disease is spread by noxious air.
From the late 1850s, hospital planning was influenced by Florence
Nightingale’s recommendation of cross-ventilated pavilion wards and sanitary
towers separated by airy lobbies. Although miasma theory was outmoded from the
1880s by the acceptance of germ theory, the modern principle that disease is
spread by bacteria, the tenets of pavilion planning continued to be widely
adopted. An increasing focus on eliminating germs led to the redecoration of
hospital spaces with smooth, impermeable and easily cleaned surfaces. Like
other institutions of its kind, the hospital installed new manufactured and
sanitary finishes such as terrazzo flooring, Opalite wall tiles, and linoleum.
The discovery of Röntgen rays and the invention of the Finsen lamp in the
1890s led to the formation of specialized departments for radiography and
light treatment. Alterations to the main hospital building were carried out in
parallel with the construction of purpose-built blocks to accommodate
specialized departments, including an outpatients’ department, an isolation
block and a laundry. This ambitious building programme relied on the
resourcefulness of the hospital’s chairman, Sydney Holland, the second
Viscount Knutsford, to attract donations. Holland was elected to the
chairmanship in 1896, and in the following year the Prince of Wales Hospital
Fund (later known as the King’s Fund) offered an annual subscription of £5,000
on condition that the hospital would spend £100,000 of its own capital on
making its buildings ‘up-to-date and efficient’.
Rowland Plumbe
In 1883 the House Committee decided to abolish the position of consulting
architect and seek advice from ‘various persons from time to time instead of
keeping to their own officer’. In the following year Plumbe was requested
to draw up plans for a large extension to Old Home, the nurses’ home adjoining
the east wing (XREF). Plumbe was an experienced architect with local origins.
He was born in 1838 in Goodman’s Fields, where his parents managed a business
selling arrowroot for medicinal use. The Plumbe family had links with the
Wycliffe Chapel in Philpot Street; his father served as a deacon at the chapel
and was a friend of its minister, Dr Andrew Reed. Plumbe studied architecture
under T. L. Donaldson at University College London and was articled to N. J.
Cottingham and Frederick Peck, followed by an interlude with F. C. Withers in
America. After returning to London in 1860, Plumbe started working as an
architect from Tokenhouse Yardin the City, establishing an extensive and
varied practice. Plumbe developed an interest in medical buildings, taking on
commissions at Poplar Hospital, St Mark’s Hospital and the National
Orthopaedic Hospital. Despite its fruitfulness and longevity, Plumbe’s
association with the London Hospital was not formalized till 1906 by his
appointment as consulting architect and election to serve on the House
Committee. Plumbe’s involvement in the hospital’s affairs continued till his
death in 1919 at the age of eighty-one. A bronzed terracotta bust by Sir
George Frampton, a gift from one of Plumbe’s daughters, was subsequently
placed in the surveyor’s office of the works department.
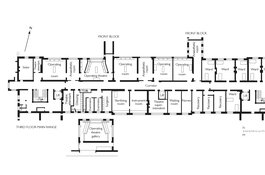
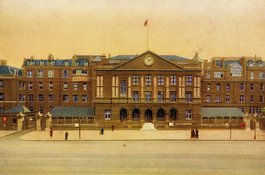
Front Block, 1890–1
The front block, built in 1890–1 by Perry & Co., was intended to improve
the practicality of the central block, yet also to bestow the hospital with a
dignified public entrance. A five-bay arcade provided a porte cochère for
horse-drawn ambulances, with sloped side approaches and a central stepped
entrance for pedestrians. The principal storey was occupied by a chapel,
expressed externally by round-arched traceried windows. The composition was
crowned by a pediment with a clock, and flanked by a pair of pavilion towers
with pyramidal roofs and finials. The front block was designed to remedy
a number of deficiencies in the central block, including the obstruction of
the main corridors by the double-height chapel and the impracticality of a
stepped entrance for emergency cases. The operating theatre and space for
clinical teaching were also outdated due to the rising number of operations
and the implementation of anaesthetics and sterile surgical techniques.
The porte cochère opened into a vestibule with a porter’s box and an office
for medical students. A hallway beyond provided access to a waiting room,
examining rooms and a receiving room. The upper floors were separated from the
central block by a light well. The first floor of the front block contained a
new chapel, furnished with a pulpit, seats and chancel furniture from its
predecessor. A five-light stained-glass memorial windowby Arthur J. Dix,
depicting ‘Christ Healing the Sick’, was donated by Emily Mary Coope in memory
of her husband Octavius Edward Coope, the local benefactor and brewer.
Dormitories for nurses and servants were in the attic storey. The transferral
of the chapel to the front block enabled the reconfiguration of the upper
floors of the central block, including the provision of a clinical lecture
theatre and an operating theatre on the second floor.
These building works were undertaken in collaboration with Dr Louis Parkes, a
leading sanitary expert engaged as assistant professor of hygiene at
University College London. The hospital’s matron Eva Lückes had raised
concerns about conditions in 1889, after observing illness among the nursing
staff. The matron’s observations were reinforced by reports of blood poisoning
and infected wounds among patients. Parkes was appointed to consider ‘every
sanitary detail connected with the hospital’, and submitted an exhaustive
report in 1890. The hospital resolved to carry out the most critical
recommendations, including the removal of old brick sewers and the
construction of a new drainage system formed of salt-glazed pipes with
manholes and traps. Parkes stressed the importance of building sanitary towers
to the east wing, the west wing and the Alexandra Wing, each containing baths,
water closets and sink rooms. He also recommended the replacement of ceiling
ventilators with Tobin’s tubes in the old wards, the installation of sash and
hopper windows, and redecoration with impermeable surfaces such as glazed
tiles and linoleum. After examining the improvements in 1893, Parkes concluded
that the work had been ‘exceedingly well done’. Between 1888 and 1894 the
hospital invested approximately £38,000 on building works, including £18,560
on the front block. The addition of sanitary towers cost £7,616, while £8,000
was spent on other improvements. Outbuildings at the east end of the hospital
were reconstructed by Perry & Co. to provide a Jewish mortuary (or Bet
Taharah),a new carpenters’ workshop, a destructor and a disinfector.
Remodelling and extension of the main hospital building, 1899–1905
The front block extension and sanitary improvements were the first components
of an extensive building programme overseen by Plumbe. The works intensified
between 1899 and 1905, when each portion of the hospital was remodelled and
extended. The scale and scope of the works were determined by 1901, when the
House Committee announced plans to enlarge and reconfigure the hospital and
construct a number of purpose-built blocks in its vicinity, including an
outpatients’ department, a post mortem department, an isolation block, and a
laundry. The estimated cost of £370,000 was described as ‘huge but absolutely
necessary expenditure’, yet it was calculated that the final cost reached
nearly £410,000.
Not a single patient bed was closed during the building works, owing to the
construction of temporary buildings in the hospital’s gardens. A single-storey
iron building containing wards for ninety-eight patients and space for the
photographic and X-ray departments was constructed in 1898–9 by the Bermondsey
builder William Harbrow, who claimed a specialism in iron buildings. This shed
also contained the hospital’s first Finsen lamp, a pioneering light radiation
machine designed to treat lupus vulgaris, a tuberculous skin infection. The
lamp was named for its Danish inventor and Nobel laureate Niels Ryberg Finsen,
and donated by Queen Alexandra in 1900. Another temporary building was
assembled on the house governor’s garden in 1899–90 to provide space for the
outpatients’ department. This shed was constructed by Humphreys of
Knightsbridge, a leading supplier of prefabricated iron hospitals. Both
buildings were demolished in 1905.
Central block and front block
Significant alterations were undertaken in the central block and the front
block by Perry & Co. between 1900 and 1903, after the acceptance of a
tender of £61,380. Building works proceeded immediately, commencing with the
underpinning and strengthening of the walls in preparation for two new
storeys. Spacious top-lit well staircases were inserted at the east and west
ends of the wing, connected on each floor by the existing corridors. Each
staircase lobby contained separate lifts for passengers and dead bodies, along
with sink rooms and water closets. In the basement, the kitchens and the
porter’s offices were replaced by dormitories for the housekeeping staff and
laundry maids. A boiler room was installed for supplying hot water and
sterilized air to the operating theatres. The ground-floor receiving room was
extended and remodelled, and most of the chapel was converted into staff
dormitories and a clinical theatre. A redecoration scheme included the
application of mosaic floors by Diespeker & Co. over the main lobby and
the receiving room, and linoleum in the main corridor.
The third-floor extension secured an extensive operating department containing
a large theatre for teaching demonstrations, four operation rooms, and
adjoining anaesthetic rooms. Only one operating theatre and three operation
rooms were intended initially, but a modification to the building contract
secured an extra suite. The department was arranged along the north side of
the central block, with large windows forming a rambling sequence of glazing
that has not been altered substantially. A top-lit corridor divided the
operating suites from a series of south-facing offices, including examination
rooms, waiting rooms, surgeon’s offices, and rooms for instruments and
sterilization. Recovery rooms were conveniently flanked by rooms for sisters
and nurses, who were also allocated bedrooms on the fourth floor. The £13,000
cost of the operating department was donated anonymously by Benjamin (or Benn)
Wolfe Levy, a businessman and philanthropist, on condition that the theatres
were ‘open to every poor patient irrespective of creed or nationality’. Levy’s
generosity was commemorated by a plaque erected after his death in 1908. A
flat roof was fitted with water tanks with a capacity of 10,000 gallons,
approximately a day’s supply for the hospital.
East wing and west wing
Plans for the remodelling and extension of the east wing were approved in
1901. The work was carried out by Perry & Co. in collaboration with W. G.
Cannon & Sons as hot water engineers and James Slater & Co. as
ventilating engineers. Works commenced with the underpinning and strengthening
of the spine walls with stanchions for the construction of two new storeys.
The basement laundry was transferred to a purpose-built detached block, and
its former rooms converted into porters’ accommodation. A number of
alterations were effected to improve ventilation in the wards, including the
enlargement of windows and the raising of ceilings on the second floor. The
insertion of openings between the back-to-back wards provided a degree of
natural cross-ventilation. The attics were rebuilt to provide a new ward on
the third floor. The fourth-floor extension provided a new kitchen with a
scullery, pantries, offices, and an external goods lift. The south end of the
floor provided bedrooms for nurses and sisters, adjacent to Old Home.
The west wing was also extended by two storeys and its existing wards
remodelled. Plumbe’s plans were submitted in June 1901 and Perry & Co.
instructed to start work immediately. Yet the impracticality of builders
taking over the west wing, which housed the medical outpatients’ department,
swiftly became apparent. The building work was postponed till the completion
of the new outpatients’ department, and carried out in 1903–4. The basement
rooms formerly occupied by the medical outpatients’ department were converted
into a series of isolation and padded rooms for psychiatric cases and patients
requiring constant supervision. The rest of the basement was devoted to an
ophthalmic department containing specialist wards, an operating theatre, and a
refraction room for eye examinations. The wards on the upper floors were
remodelled to improve ventilation and the comfort of patients. The first- and
second-floor wards had access to external balconies, reflecting a growing
interest among medical practitioners in the beneficial effects of fresh air
and sunlight.
The fourth-floor extension was devoted to Jewish patients, with two wards
divided by a central lobby containing a kosher kitchen and a scullery. One for
men and one for women, these wards were named ‘Rothschild’ and ‘Goldsmid’
respectively. The reinstatement of dedicated Jewish wards reflected the
reality on the ground that the London Hospital was the principal hospital used
by the now significantly larger Jewish community. These wards were formally
opened in November 1902 by the prominent banker and philanthropist Leopold de
Rothschild, in his capacity as vice-president of the hospital. Other Jewish
philanthropists such as Sir Samuel Montagu and Sir Benjamin L. Cohen served on
the House Committee, organized appeals, and made personal donations to the
hospital.
Alexandra Wing and Grocers’ Company’s Wing
The external appearance of the Alexandra Wing was not much altered during the
building programme, yet its interior spaces were remodelled extensively. The
alterations were completed in 1905 by Perry & Co., with Cannon & Sons
as hot water engineers, Slater & Co. as ventilating engineers, and the
plumber R. A. Marshall. The removal of the surgical outpatients’ department
from the basement provided space for a coroner’s court with a public gallery,
a witness room and a coroner’s office. The basement also contained a massage
department and offices for the hospital’s surveyor. The ground floor was
converted entirely to administrative use, with a new committee room,
secretarial offices and an estate office. The rest of the wing was devoted to
maternity cases, with a first-floor obstetric operating theatre and a south-
facing ward with a balcony. The Marie Celeste maternity department was
formally opened on the second floor in 1905. Named in memory of the wife of
James Hora, a vice-president of the hospital, the suite contained a labour
room, an isolation room and a lecture room. Three small wards extended along
the south side of the second floor, opening onto a balcony with views over the
rear garden. The attic dormitories were assigned to the maternity staff and
pupil midwives. The Grocers’ Company’s Wing was altered on a
comparatively modest scale. South-facing ward balconies were installed and
windows were enlarged and fitted with patented ‘Luxfer’ prism glass to
maximize light. The basement was reconfigured to form a large surgical ward
for male patients, and the ground floor contained a female surgical ward
equipped with an operating suite. These alterations were completed in
1905.
Gardens and forecourt
Plans were produced for redesigning the gardens in 1906, after the building
works created a state of disarray. The rear quadrangle was bestowed with a
bronze statue of Queen Alexandra created in 1907–8 by George Edward Wade, a
favoured sculptor among the royal family. The statue commemorated her
longstanding support of the hospital and consent to serve as its president, a
title she retained from 1904 to her death in 1925. Alexandra agreed to pose
for the sculpture, which depicts her standing with dignified composure,
holding a sceptre in her right hand. She is garbed in coronation robes, her
state crown, jewels and a pearl necklace. The robust stone plinth has an
inscribed bronze plaque and a bronze bas-relief panel depicting a royal visit
to the Finsen light department in the outpatients’ department. At the centre
of the composition, Alexandra bends to observe a patient receiving treatment
with the use of a Finsen lamp. She is accompanied by King Edward VII and an
entourage of representatives of the hospital, including its chairman Sydney
Holland, the surgeon Sir Frederick Treves, and the matron Eva Lückes. Wade’s
statue is currently positioned on the south side of Stepney Way, in an
incongruous spot beneath the canopy of the new hospital.
In its original position on a raised plinth at the centre of the quadrangle,
the statue was encircled by an asphalt path with straight offshoots leading to
the central block, the east wing and the west wing. A pair of timber shelters
for patients was positioned at the south end of the quadrangle, screening it
from the open ground on the north side of Stepney Way. A porter’s lodge was
also built at the south-east corner of the garden. Perry & Co. were
contracted to construct the lodge and the shelters, along with the weighty
stone pedestal of the statue. The narrow wedge-shaped courtyard to the east of
the hospital, known colloquially as ‘Bedstead Square’ for its proximity to the
steward’s stores, was decorated with planters gifted by the local brewing firm
Mann, Crossman & Paulin. Timber shelters were also built on the forecourt
of the hospital to accommodate patients’ relatives and friends, these
constructed in 1912 by Perry & Co. to designs by J. G. Oatley.
Additions and alterations in the twentieth century
Contributed by Survey of London on April 29, 2019
The rebuilding and expansion of the hospital under Plumbe’s supervision
created a large medical complex that functioned on modern and efficient lines,
requiring few alterations for some time. The important work of the hospital
during the First World War has been chronicled in the second volume of A. E.
Clark-Kennedy’s institutional history. After emerging from the war in
significant debt owing partly to higher wages and the rising cost of medical
treatment, the hospital opted to introduce a fee of 10s. per week for
inpatients who could afford it. This shift from the institution’s policy of
providing treatment without any charge to its patients was bolstered by the
Insurance Act of 1911, which protected workers from a loss of earnings during
illness. The hospital was associated with discussions over the organization of
healthcare through its physician Lord Dawson of Penn, whose 1920 report
foreshadowed the establishment of the NHS. Despite the introduction of patient
fees, the hospital’s finances were so troubled that 200 beds were closed
temporarily in 1921. Approximately half of these beds were reopened after a
fundraising appeal in 1923, but the rest were sacrificed to provide space for
specialist equipment, offices and staff accommodation, leaving a total of
approximately 850 beds in the hospital.
Interwar alterations
The interwar period witnessed few substantial alterations to the main hospital
building, owing to financial struggles and the longevity of the improvements
made by Plumbe. The works department was headed by J. G. Oatley, who continued
as hospital surveyor till his retirement in 1933. He was succeeded by his son,
Norman Herbert Oatley, who served until the 1950s. Most alterations were
precipitated by the installation of specialized departments, which multiplied
in general hospitals after the First World War. By 1926, the hospital
contained eighteen operating theatres and fourteen specialized departments.
The central block and the front block were the focus for alterations in the
main hospital building, but a number of departments were established in
purpose-built detached blocks in the immediate vicinity. The clinical theatre
adjacent to the chapel in the front block was transferred to the Bearsted
Clinical Theatre to provide space for laboratories, and all but one of the
traceried windows were replaced with a series of workmanlike apertures. A
gynaecological operating suite was installed on the third floor of the central
block, with a bay window that survives on the north front. This facility was
funded by a donation from Louis F. Stanton Bader, a coal dealer of Boston,
USA, in gratitude for the treatment of his wife by the obstetric surgeons
Russell Andrews and Eardley Holland. In 1929, a radium laboratory was
installed on the second floor of the front block.
A covered way was constructed in the quadrangle by William Wood & Sons of
Taplow in 1929–30. The pergola extended from the rear entrance of the central
block along the east side of the garden, providing shelter for patients and
staff. It was financed by Sir William Paulin, the honorary treasurer of the
hospital. A memorial tablet designed by Edwin Lutyens was unveiled in the
front hall in 1933 to commemorate Sydney Holland, the hospital’s chairman.
Isolation wards were installed in the Grocers’ Company’s Wing by Walter
Gladding & Co. in 1935, facilitating the conversion of the Fielden
Isolation Block to wards for private patients.
Post-war rebuilding schemes and extensions
Contributed by Survey of London on April 29, 2019
In 1940 a bicentenary campaign was launched for a programme of repair and
reconstruction. The earlier building works overseen by Plumbe were commended
for their solid construction and spacious planning, which obviated the need
for large-scale redevelopment. The hospital required new departments to pursue
advances in medicine, such as dietetics, blood analysis and psychology.
Research was restricted by a lack of space and the dispersal of laboratories
around the hospital. William Goschen, the hospital’s chairman, urged that it
would be ‘impossible to keep pace with modern developments without an
extensive scheme of reconstruction’. In the first phase of the proposed
scheme, the clearance of attic nurses’ dormitories was intended to provide
room for clinical laboratories and new aural wards. Later phases promised to
secure improved facilities for the radiology department, a new wing for a
casualty department and fracture clinic, wards for infected surgical cases,
and a new genito-urinary clinic, dental department and light treatment clinic.
The hospital also intended to modernize the operating theatres and the general
wards.
The bicentenary programme was abandoned due to the onset of the Second World
War, which plunged the hospital into preparations for air raids and
casualties. In 1940, the Alexandra Home, the Eva Lückes Home and the medical
college were hit by bombs. The hospital evaded severe destruction until August
1944, when the east wing was damaged severely by a V-1 flying bomb. The
hospital also emerged from the war in significant debt, with meagre hope of
repairing bomb damage and carrying out improvements without assistance from
the state. The establishment of the NHS in 1948 brought the hospital under the
administration of a board of governors that reported to the Ministry of
Health. All patient fees were eliminated and salaries introduced for the
medical staff, who had previously devoted their time to the hospital as
honorary consultants while maintaining private practices elsewhere.
Two ambitious rebuilding schemes were mooted after the Second World War. The
first proposal by Adams, Holden & Pearson, drawn up in 1947, was not
implemented due to limited funds, and the second scheme by T. P. Bennett &
Son was drastically curtailed in the 1970s by the listing of historic
buildings. The unexecuted scheme of 1947 proposed to extend the hospital’s
footprint southwards to Varden Street, producing an extensive and functional
teaching hospital with 1,000 beds. The main hospital building was to be
remodelled to contain administrative offices, laboratories, and wards in the
Alexandra Wing and the Grocers’ Company’s Wing. The southern portion of the
hospital complex was to be mostly cleared for new buildings. A low-lying
receiving block and accident department, flanked by medical and surgical ward
wings, was designed to provide a new public entrance to the hospital. An
operation block was planned for the site of the medical college, adjacent to a
rehabilitation department and surgical wards. Extensions to the Edith Cavell
Home and the Eva Lückes Home were intended to accommodate more than 700
nurses. A scattering of buildings on the hospital’s estate, including St
Philip’s Church and the students’ hostel in Philpot Street, were to be
preserved and engulfed by a series of uniform buildings grouped to provide
distinct quarters for outpatients, inpatients and the medical college.
In the event, inflation put paid to these plans for redevelopment. Post-war
alterations and additions proceeded in a piecemeal manner, based on the
framework set out in the bicentenary campaign. The works department embarked
on numerous alterations in the years immediately after the war. A new
receiving and accident department was formed in the front block, along with
first-floor research laboratories replacing children’s wards on the south side
of the central block. These laboratories were assigned to bacteriology and
industrial diseases. Additional works were carried out in 1952–3,
including the formation of a genito-urinary department, alterations to the
laundry, and the enlargement of the dental division of the outpatients’
department.
The most significant alterations to the main hospital building in the 1950s
were carried out by W. H. Watkins, Gray & Partners, an architectural firm
with substantial experience of hospital work. Watkins, Gray & Partners
worked in association with the hospital’s surveyor R. M. Halsey, who succeeded
Oatley. The upper storeys of the bomb-damaged east wing were rebuilt in
1958–9, followed by a five-storey extension to the west wing to provide
additional wards. Bennett & Son oversaw further alterations to the main
hospital building, along with the construction of the Holland Wing and the
rebuilding of the Alexandra Wing. Leonard Abbott, an associate (1966) then
partner (1973) in the firm, supervised the works due to his specialism in
hospitals. The main public entrance to the hospital was altered around 1969 by
the application of marble cladding. Bennett & Son also developed
proposals for the rebuilding of the hospital on expanded lines, with large
blocks engulfing the eastern side of its estate. This fifteen-year project
aimed to raise the size of the hospital from approximately 750 beds to 1,300
beds by 1972. The scheme was partially realised by the construction of
Knutsford House, the Institute of Pathology, the Princess Alexandra School of
Nursing, John Harrison House, a computer centre, and a cluster of nurses’
homes. The listing of the main hospital building in 1973 thwarted plans for
its redevelopment, and only the Alexandra Wing was rebuilt.
Link Block, 1959–62
The post-war building programme encroached on many of the open spaces
surrounding the hospital. The quadrangle was mostly sacrificed for the Link
Block in 1959–62. This six-storey extension was designed by Watkins, Gray
& Partners in association with R. M. Halsey and consulting engineers Oscar
Faber & Partners. The block provided additional wards and kitchens,
connecting the west and east wings. The upper floors were elevated by a series
of reinforced-concrete piers to preserve a route between the remainder of the
quadrangle and the hospital’s gardens. The north and south elevations
incorporated metal-framed projecting balconies, breaking the monotony of sheer
expanses of brickwork. Single-storey clinics for dialysis and radiology,
flanking the ground-floor passageway, were added by Bennett & Son in
1967–8.
Holland Wing, c.1968
The Holland Wing, named after the hospital’s longstanding chairman, replaced
the southern portion of the Grocers’ Company’s Wing and the Bernhard Baron
Pathology Institute in the late 1960s. This five-storey block designed by
Bennett & Son was described in design stages as a ‘decanting building’, a
name that captured its assorted administrative, medical and teaching
functions. The block was positioned on the west side of East Mount Street,
with brick-clad elevations divided by horizontal bands of glazing and mosaic.
Each floor contained a central north–south corridor, extending from the
Grocers’ Company’s Wing to a lift lobby at the south end of the block. The
internal spaces were divided by partition walls to ensure future adaptability.
A cardiac department was installed in the basement, and the ground floor
contained staff offices and a board room. The first and second floors were
devoted to a maternity department, composed of delivery suites, isolation
rooms, and four-bed wards with ancillary rooms. An intensive neonatal unit was
located on the third floor. The fourth floor contained research laboratories
and facilities for the medical college, including a library and a conference
room.
Conversion to a Town Hall
Contributed by Survey of London on April 29, 2019
At the time of writing (2021), the former hospital is in the throes of
adaptation and extension to provide a new town hall for Tower Hamlets Council.
This major redevelopment scheme has been in genesis for a number of years,
prompted by the looming expiration of the lease of the council’s headquarters
at Mulberry Place in East India Docks. In 2013 the council produced a
feasibility study for a town hall, concentrating on the former hospital and a
site in Commercial Road. The hospital was vacant after the completion of its
new premises, and gained preference. A significant factor was its location
nearer the geographical centre of the borough, which presented an opportunity
to reconfigure public services and council offices on a prominent and
accessible site. The council intended to dispose of other bases in the borough
to raise funds for the conversion of the hospital, which is likely to reach
£115m. By operating only from the new town hall and John Onslow House towards
the northern extremity of its jurisdiction in Bow, the council anticipates
savings and efficiencies. The reuse of the hospital also forms a major
component of Whitechapel Vision, the council’s scheme for local
regeneration.
Ian Chalk Architects (ICA) were appointed to produce a brief for the project,
which was intended to form the basis of an invitation to tender. The initial
proposal established a broad concept for the works. The main hospital building
had been mutilated during the construction of the new hospital, with the
clearance of the east wing and the Holland Wing. ICA recommended the retention
and refurbishment of the surviving north front of the main hospital hospital
in Whitechapel Road, including the Grocers’ Company’s Wing. The rear of the
central block and the west wing were to be cleared for a new building. The
site was purchased from Barts Health NHS Trust for £9m in 2015.
In the following year, a team of consultants led by architects Allford Hall
Monaghan Morris (AHMM) was appointed to develop the proposal. AHMM was
selected to lead the initiative after a competition between six bidders
invited to submit tenders. The winning team included Elliott Wood as
structural engineers, Gerald Eve as planning consultants, Kinnear Landscape
Architects, and Richard Griffiths Architects as heritage consultants. The
brief was adjusted gradually to maximize space and increase the number of
workstations to accommodate a workforce of approximately 2,500 employees. A
reworking of the scheme proposed to replace the Grocers’ Company’s Wing with a
modern block fronting Whitechapel Road, yet this was revised after objections
from Historic England.
A later proposal, which gained planning permission in 2018, accords with the
initial scheme drawn up by ICA in the retention of the main range of 1752–9,
the front block of 1890–1 and the façade of the Grocers’ Company’s Wing of
1873–6. The clearance of the west wing has made way for a significant rear
extension comprising two modern blocks connected by a link block with a roof
terrace. The height of the seven-storey west block was dictated by the scale
of the adjoining dental hospital, while the four-storey east block was
designed to lurk behind the Grocers’ Company’s Wing. The raised basement of
the Grocers' Wing will be converted into a public entrance accessed from
Whitechapel Road, faced with large expanses of glazing interspersed with steel
columns. The new blocks are set to be clad with brickwork piers and glazed-
brick panels, while the link block will be cocooned in aluminium curtain
walling in colourss inspired by surviving fragments of terrazzo flooring.
The town hall has been planned to accommodate a mixture of public amenities,
council services and staff offices. The ground floor has been envisaged as a
public space, containing a reception, a café, libraries, housing advice
offices and a council chamber. The upper floors will be devoted to staff
offices, including open-plan spaces, executive offices and meeting rooms. An
atrium forms a narrow cleft between the main range of the hospital and the
modern blocks, which are linked by bridges. The haphazard fenestration on the
north front of the hospital, the outcome of successive alterations, will be
retained. The original fenestration of the south front of the main range will
be more legible, with the removal of balconies and other functional additions.
AHMM intends to reuse hospital spaces, converting the former chapel into a
staff refectory and the third-floor operating theatres into offices and
meeting rooms. A prayer room will be behind the clock pediment of the front
block. The east and west staircases of the central block will be retained as
core spaces for circulation, lifts and sanitary facilities, a function
curiously aligned with their original purpose in the hospital. The
construction work uncovered original Serlian windows at the east end of the
main range, along with steel beams and stanchions inserted as part of the
remodelling and structural reinforcement of 1900–3. AHMM intends to retain the
visibility of these historic traces in the finshed scheme. Preparatory works
were started in 2018 by main contractor Bouygues, and completion is scheduled
for 2022. A masterplan for a public square to the south of the civic centre is
set to be prepared in collaboration with Barts Health NHS Trust.
Staff Accommodation
Contributed by Survey of London on April 29, 2019
In the eighteenth century, nurses were confined for their rest to tiny rooms
in lobbies adjacent to the wards. This arrangement was customary in general
hospitals and persisted at the London Hospital until the 1860s, with minor
improvements. The ward lobbies in the east and west wing extensions of 1830–42
incorporated larger bedrooms, kitchens, washing rooms and bathrooms. At this
time, attic bedrooms in the central block were assigned to assistant nurses,
laundry maids and ‘watchers’, or night nurses. Bedrooms were also provided for
the cook, the clerk and the surgeon’s assistant. Senior employees enjoyed a
greater level of comfort, with separate apartments assigned to the house
governor, the apothecary, the matron and the head nurse.
By the mid nineteenth century, the provision of nurses’ accommodation was
deficient owing to the swift expansion of the hospital and its rising
population of resident staff. The 1841 census recorded a nursing staff of only
37, whereas the 1851 census calculated 57 nurses. By the 1860s, the provision
of sleeping quarters was considered essential to preserving discipline and
respectability among nurses, who were drawn predominantly from the working
classes. For instance, the absence of dormitories was deemed to ‘lower the
standard of the women who can be obtained for night duty’ and diminish their
efficiency. The attics of the Alexandra Wing (1864–6) secured four
communal dormitories for night nurses and household staff. Despite this
addition, nurses were accustomed to ‘boxing and coxing’, or occupying beds at
different hours between shifts. In contrast, the house governor lived in a
three-storey maisonette with servants’ quarters and a private walled garden.
By 1871, there were 52 nurses and 23 night nurses residing in the hospital,
and other nurses living in the vicinity. Only a short time elapsed before
plans for the Grocers’ Company’s Wing necessitated more than thirty additional
nurses, prompting significant improvements to accommodate an expanded nursing
staff of as many as 154. An extension to the east wing provided the first
purpose-built residential home for the nursing staff, containing dormitories,
dining rooms, and a suite of rooms allocated to the matron.
This advance established the pattern for subsequent additions to the
accommodation for nurses. Four purpose-built homes were erected on and
adjacent to the hospital’s grounds between 1884 and 1918: Old Home (1884) and
Alexandra Home (1895–6) were connected to the east wing, while the monumental
Eva Lückes Home (1903–5) and Edith Cavell Home (1915–8) were located in
Stepney Way and East Mount Street respectively, and accessed by covered
bridges. This energetic building programme was propelled by reforms to the
nursing system carried out under the guidance of Eva Lückes, the hospital’s
matron from 1880 to her death in 1919. During her long incumbency, she
introduced new measures to improve the training and education of nurses, along
with their living and working conditions. Lückes started a course of lectures
for probationers in 1881, and established a training school for aspiring
probationers in 1895. The construction of purpose-built nurses’ homes was
integral to Lückes’s efforts to raise the standard of nursing. The provision
of individual bedrooms reflected her instinct that ‘separate apartments,
however small, are absolutely essential, both on grounds of comfort and
discipline’.
The preservation of health, respectability and discipline among the nursing
staff provided the main impetus to build residences on and adjoining the
hospital’s grounds, and shaped their configuration. The number of nurses
increased significantly under Lückes’s supervision. The 1881 census recorded a
resident nursing staff of 87, while the 1911 census counted 446 nurses.
Covered bridges extended between the tall blocks of the nurses’ quarter to
ensure safety, convenience and protection from bad weather. Bedrooms allocated
to sisters, or senior nurses, were interspersed between nurses’ dormitories to
secure a degree of surveillance. Despite these authoritative measures, the
nurses gained several amenities for their enjoyment and relaxation. Their
homes contained a range of leisure spaces, including dining halls, sitting
rooms and libraries. A public garden in Stepney Way was also provided for the
diversion of nurses, who referred to it affectionately as ‘the Garden of
Eden’. The addition of an indoor swimming bath at the east end of the garden
in 1936–7 was another boon.
The swift construction of the nurses’ homes produced a sprawling residential
quarter drifting south from the main hospital building, marked by tall,
austere blocks connected by covered bridges. Despite this advance, a large
number of staff, including nurses, continued to reside in the main hospital
building. After the completion of the building programme in 1906, staff
accommodation was dispersed throughout the hospital. The degree of comfort
continued to be dictated by seniority. Laundry maids slept in basement
dormitories, while maternity students and night dispensers were allocated
first-floor rooms. The attics of the front block, the east wing, and the
Grocers’ Company’s Wing contained bedrooms for nurses, while trainee midwives
and maternity staff had attic bedrooms in the Alexandra Wing. Cooks slept in
the attics of the east wing, adjacent to the kitchens. Resident physicians and
surgeons enjoyed the privilege of private apartments containing a bedroom and
a sitting room. Receiving room officers acquired similar amenities by the
rebuilding of 72–74 New Road in 1903–4, but were subsequently transferred to a
resident doctors’ hostel on the south side of Mount Terrace. Despite the
generous provision of hospital accommodation, many employees continued to
reside in private lodgings. Gwynne House in Turner Street, a block of compact
flats with a resident caretaker, was immediately popular among staff and
students at its completion in 1938, and later acquired by the hospital as
rented accommodation.
After the Second World War, large swathes of the hospital’s estate were
cleared as part of the redevelopment scheme produced by Bennett & Son. An
extension to the Edith Cavell Home had been envisaged in the late 1930s, and
the scheme was revived as Knutsford House (1957–9), a block of apartments
rented to senior nurses. The ruins of the bombed-out Great Synagogue
(previously the Wycliffe Chapel) on the east side of Philpot Street were
cleared for John Harrison House (1962–4), a ten-storey tower blockwith 227
bedsitting rooms for nursing and administrative staff. Bennett & Son also
produced plans to clear a large site for a cluster of nurses’ homes set in
landscaped gardens. This scheme was partially executed with the construction
of a block of flats and dormitories around Varden Street, opened formally in
1976. Plans for the new hospital precipitated the large-scale demolition of
the first wave of nurses’ homes. Old Home, Alexandra Home, Eva Lückes Home,
and Cavell Home were cleared, eradicating the concentration of nurses’ homes
constructed between 1884 and 1918. Knutsford House was also demolished at this
time, while John Harrison House has largely been converted to administrative
offices. The group of 1970s nurses’ homes around Walden Street has survived,
but the population of hospital employees has declined after the majority of
the blocks was sold to a private developer.
Old Home (1875–6)
Contributed by Survey of London on April 29, 2019
Plans for the Grocers’ Company’s Wing gave rise to a scheme for the hospital’s
first purpose-built nurses’ home, intended to provide dormitories and
recreation rooms for an expanded staff. In 1874 the house governor, William
Nixon, estimated that the enlarged hospital would require more than thirty
additional nurses (including sisters, probationers, day nurses and night
nurses). Nixon proposed that the resident medical officers should be allocated
rooms in the central block, and a new building constructed to house the
matron, the steward, and nurses. The most suitable position for the building
was deemed to be at the south end of the east wing, where communication with
an earlier staircase lobby would ensure proximity to the main hospital
building. Plans were prepared in rough by J. A. Thornhill and finished by
Charles Barry Jr, who received instructions not to exceed an estimate of
£5,900. A high tender from Perry & Co. was reduced to £6,168.10, and
construction followed in 1875.
The result of this economy was an austere brick building composed of four
storeys above a raised basement. A pediment on its west façade echoed the
articulation of the lobbies at the centre of the east and west wings.
Notwithstanding modest appearance, this residence improved conditions for the
hospital’s nursing staff. A few years earlier, Nixon had observed that nurses
suffered frequently under the strain of ‘constant overwork’, without rooms for
relaxation. The home provided a dormitory for thirty-five nurses, along
with separate accommodation for probationers. A recreation room and a
dining room were also provided above the matron’s apartment, an arrangement
intended to ensure supervision ‘without any appearance of intrusive
watchfulness’.
The nurses’ home was subsequently extended to designs by Plumbe, with the
construction of a six-storey block with dormitories for approximately 100
nurses and a two-storey residence for the steward. Small individual nurses’
bedrooms were crammed into a narrow rectangular plan with a central corridor.
Water closets, sinks and bathrooms on each floor were confined to a projecting
sanitary tower. A three-bay staircase range linked this block with the earlier
nurses’ home, where dormitories were converted into dining rooms, sitting
rooms and visiting rooms. Its brick-built exterior matched the austerity of
the earlier hospital buildings, with decoration limited to iron balconies,
crow-stepped gables, and a corbelled cornice of moulded brickwork. The
extension was built by William Goodman and opened formally by the Prince and
Princess of Wales in 1887.
Chaplain’s house (1886–7)
Contributed by Survey of London on April 29, 2019
Built in 1886–7 by Goodman to designs by Plumbe, this large detached house
provided comfortable living quarters for the hospital chaplain in close
proximity to his duties. A handsome west front incorporated a stepped entrance
porch and a bay window with views over the hospital’s gardens. A kitchen and
servants’ quarters were provided in a raised basement and a steeply pitched
roof with dormer windows. The house lost its detached status by the
construction of the Alexandra Home to the east in 1895–6. After the Rev.
Sidney Vatcher, the incumbent of St Philip’s Church, assumed control of the
hospital’s chaplaincy in 1898, the residence was converted into a temporary
isolation block to accommodate infectious patients. It was demolished around
1915 to make way for the further enlargement of Alexandra Home.
Alexandra Home (1895–6)
Contributed by Survey of London on April 29, 2019
The provision of nurses’ accommodation was extended significantly by the
construction of the Alexandra Home in 1895–6 by William Shepherd to designs by
Plumbe. This tall six-storey block was positioned at the crossing between
Stepney Way and East Mount Street, abutting the chaplain’s house to the west.
With its utilitarian and neatly fenestrated stock-brick elevations, the
Alexandra Home matched the austerity of Old Home, with which it was linked by
a covered bridge. Plumbe adopted a similar plan to the earlier home, squeezing
around ninety bedrooms into an L-shaped footprint. On each dormitory floor a
series of single-bay bedrooms for individual nurses flanked a central
corridor. A projecting sanitary tower at the north-east corner of the block
contained bathrooms, water closets, sinks and fire escape staircases. The
attics contained wooden lockers allocated to the nurses. A six-storey west
addition of about 1915 designed by J. G. Oatley provided larger bedrooms for
sisters with access to bathrooms and hair-washing rooms, a luxury introduced
contemporaneously at Edith Cavell Home.
Eva Lückes Home (1903–5)
Contributed by Survey of London on April 29, 2019
Built in 1903–5 by F. Gough & Co. of Hendon to designs by Plumbe, Eva
Lückes Home was a sprawling five-storey block with a U-shaped plan, comprising
a north range fronting Stepney Way and an extensive south range overlooking
Newark Street, linked by an intervening corridor range. The Lückes Home
replaced a substantial portion of the hospital’s estate, including the British
Oak Public House, to provide more than 270 nurses’ bedrooms. Decoration was
restricted to gables with diaper patterns, a moulded brick cornice, and
shallow bow windows set within relieving arches. A porch facing Stepney Way
opened into an entrance hall leading to various offices, a visiting room, a
writing room and a sitting room. An iron and concrete covered bridge over
Stepney Way linked the nurses’ home with the Alexandra Home opposite. Plumbe
repeated the configuration deployed at Old Home and Alexandra Home, dividing
each dormitory floor into compact single-bay bedrooms and larger bedrooms with
fireplaces for sisters. Bathrooms and water closets were confined to sanitary
towers at the east end of each range. A basement provided servants’ bedrooms
and a sitting room. The attic was reserved for a locker room, a linen room and
water tanks.
Edith Cavell Home (1915–18)
Contributed by Survey of London on April 29, 2019
Edith Cavell Home was positioned at the north-east corner of the junction of
East Mount Street with Stepney Way. At its completion, this six-storey block
provided 122 bedrooms for nurses and sisters. Construction by Perry & Co.
was delayed by the First World War, yet nurses eventually moved into Cavell
Home in June 1918. The clearance of terraced houses provided a narrow
rectangular site for this addition to the nurses’ accommodation. A stone porch
with neo-Baroque flourishes departed from the austerity of the earlier nurses’
homes, hinting at delegation by Plumbe. The customary arrangement of small
bedrooms flanking a central corridor suited the constraints of the site. The
ground floor had a sitting room, a library and a visiting room, along with
bedrooms for sisters and nurses, while a basement contained servants’
quarters. Accessed by a central lift and a well staircase, each dormitory
floor contained twenty nurses’ bedrooms and two larger bedrooms for sisters,
who enjoyed the comfort of a fireplace. Water closets were confined to a
sanitary tower at the rear of the block. Bathrooms, hair-washing rooms, and
linen cupboards were positioned at the north end of each floor, adjacent to a
subsidiary staircase. On the second floor, a covered bridge extended across
East Mount Street to Old Home. The hospital named the home in honour of Edith
Cavell, the British nurse executed in October 1915 for assisting the escape of
allied soldiers from German-occupied Brussels. Cavell had trained at the
hospital as a probationer in 1896–8 and served on the institution’s private
nursing staff until 1901. A plaster bust of Cavell by Sir George Frampton was
placed in the sitting room, and survives in the Royal London Hospital
Museum.
Knutsford House (1956–60)
Contributed by Survey of London on April 29, 2019
Plans to enlarge Edith Cavell Home were produced in 1939 by N. H. Oatley, who
proposed clearing the adjacent terraced houses for a six-storey extension. The
scheme was revived with a renewed specification after the war, with Bennett
& Son appointed as architects. They departed from the familiar and
established configuration of nurses’ dormitories interspersed with bedsitting
rooms for sisters. Knutsford House, a six-storey concrete-framed and brick-
faced block, opened in May 1957 to provide forty-one self-contained flats
reserved exclusively for sisters. Each flat contained a bedroom, a living
room, a kitchenette and a bathroom. A basement contained a box room, storage
lockers and laundry facilities, along with service rooms. Plans were swiftly
in hand for an addition extending north to the corner of Raven Row, securing
an additional six flats on the principal floors. The block was named in memory
of Sydney Holland, the hospital’s chairman.
Nurses’ garden
Contributed by Survey of London on April 29, 2019
The nurses’ garden occupied a large plot to the south of the hospital, bounded
by Stepney Way to the north, Newark Street to the south, and the laundry to
the east. It had originally been laid out in connection with almshouses built
for John Baker’s Charity by the Brewers’ Company, which agreed to preserve
ground directly behind the hospital as a shrubbery. The medical officers had
resisted building development immediately behind the hospital, prizing fresh
air and good ventilation. This principle was firmly established by 1814, when
an accounts committee recommended leasing the vacant, ‘unproductive’ land
behind the hospital for any purpose that would not contaminate the quality of
the air. The conveyance of the piece of ground to the Brewers’ Company
converted it to a suitable purpose, and it was enclosed for a garden
overlooked by the almshouses. By 1881 it had fallen into neglect and was
transferred to a local committee headed by the businessman Stanley Kemp-Welch
and the Rev. Sidney Vatcher of St Philip’s Church. It was redesigned and
replanted in 1882 as a public garden, with a pond, a fountain and an aviary.
Entrance gates were donated by the St Pancras Ironwork Company and a garden
house was donated by Lord and Lady Brabazon. The garden was inherited by the
hospital’s nurses in 1898, shortly after the almshouses were acquired to
provide a site for a laundry. Nurses were required to collect a key from the
hospital, which fitted the garden gate and the doors of St Philip’s Church.
After the construction of an indoor swimming bath in 1936–7, the garden was
redesigned with symmetrical footpaths dividing flat lawns and neat corner
pavilions at its west end. The garden survived until 1963, when it was cleared
for a pathology block.
Nurses’ swimming bath (1936–7)
Contributed by Survey of London on April 29, 2019
A swimming bath was built in 1936–7 on the east side of the nurses’ garden,
financed by a donation from E. W. Meyerstein, a retired stockbroker who
endowed numerous hospitals. A handful of sites on the hospital’s estate were
considered for a nurses’ swimming bath, but it was determined that the garden
possessed ‘the merit of simplicity’. The chosen position adjacent to the
laundry preserved the majority of the garden, and avoided the costly
implication of uprooting tenants. The house governor, A. G. Elliott, and
surveyor, J. G. Oatley, undertook to engage an architectural firm with
specialist experience of swimming baths. Visits were arranged to comparable
baths, including those at St Mary’s Hospital, the Middlesex Hospital, and
Bourne & Hollingsworth’s staff hostel in Gower Street. Alfred W. S. Cross
and Kenneth M. B. Cross were identified as the leading architects in the
field. This father-son partnership boasted longstanding experience of swimming
baths, including the municipal baths in Haggerston and the nurses’ baths at
the Middlesex Hospital.
Cross & Cross designed a low-lying brick-built structure with a sequence
of flat roofs serving as garden terraces. The west elevation overlooking the
nurses’ garden had a jaunty appearance, exaggerated by a series of porthole
windows. A central staircase ascended to a first-floor terrace, adorned with a
Portland stone plaque commemorating Meyerstein’s generosity. A porch at the
north end of the building served as the nurses’ entrance to the swimming bath,
opening into a passage leading to a top-lit changing area. The ground floor
was dominated by the rectangular top-lit swimming pool, skirted on its west
side by a viewing gallery with tiered seating for seventy spectators. A
reinforced-concrete basement contained a filtration plant room. Construction
by William Moss & Sons of Cricklewood commenced in July 1936, and the
swimming pool was opened in the following spring.
Air Raid Shelter during the First World War
Contributed by gelosake on April 18, 2018
My grandmother lived in the Star and Garter pub across the road from the Royal
London Hospital during the First World War. During air raids they would run to
the basement of the London Hospital for shelter.
My life in Whitechapel
Contributed by Shila_B on Sept. 13, 2017
Shila B, interviewed by her neighbour Jil Cove, August 2017:
I went to Blue Gate Fields Primary School and then to Mulberry. I really
enjoyed school and left with General National Vocational Qualifications (GNVQ)
in health and social care. I volunteered at the London Hospital until I got a
part time job there which later became full time job. I worked in admin in the
gynae department for 8 years. I loved the work and sometimes, I was asked to
use my bilingual skills if an advocate was not available.
When I was at The London there was a great fish and chip shop opposite – the
chips were fantastic and the fish was really good too. I often went there at
lunch time, it was very traditional and when the owners changed I could taste
the difference in the quality of the cooking. I really missed it when it I
stopped working and still miss it, even today; I can still taste the chips!
Sometimes after work a group of us would go to the Pizza Hut opposite, but I
didn’t miss that so much when it closed.
My marriage was arranged when I was 20 and took place in Bangladesh. I carried
on working until my first son was born; I now have 3 sons aged 16, 11 and 9.
The 16 year old has recently received his GCSE results and my husband and I
are very proud to say that he passed all eight subjects one with an A* and the
others were A’s and B’s. He is going to start college soon to study for his A
levels.
My husband is a butcher by trade but has now got heart problems that prevent
him from working. His English is rather limited though it has got better over
the years with the children speaking to him in English. At first, he was
unable to go to English classes as locally we couldn’t find one that fitted in
with his work hours and now he is reluctant to go as the ESOL classes are
predominantly for women, so he would be the only man in the class.
My dad came to the UK from Bangladesh before I was born, and I was about 6 or
7 when my mum brought me and my three brothers to join him. My eldest brother
who was 16 or 17 at the time had to stay behind because of immigration rules
but he eventually joined us about 18 months later; my youngest brother was
born here. Dad originally worked in textile factories in the north of England
and I don’t know why he moved to London. His English was always very limited
and my mum has virtually no English as she was isolated when we lived in
Shadwell and busy with looking after 6 children. She didn’t know anyone to
give her any support or guidance so never had time to learn. My dad died in
1987 and now my mum lives with my youngest brother. I’m really pleased that
she is involved in lots of activities every day enjoying various groups
including Arabic classes, and though she still has no English she is quite
independent of the family and is out and about every day.
I come from a very big extended family and we all live in the Whitechapel area
so see each other often. Just recently one of my nieces got engaged which
meant a large celebration party; about 40 members of my extended family came
along with a similar number from the soon to be groom’s family. We all had a
good time with lovely food and a very late night. I was telling my neighbour
about this and she was amazed at having such a large family and that we are
all in such close contact with each other.
I’ve lived in this same street with my family for about 15 years now and moved
with all my neighbours into a new block of flats in 2013. Though my new flat
is much bigger, I do miss the very big balcony I had before where the children
could play safely outside. I think that Whitechapel market has changed as
there are now too many clothes stalls so there is not the variety of things
any more. I tend to go to Wapping for my fish and herbs, and do the big
shopping at Iceland as they delivery to my door.
One of the downsides to living where I do, is that as a car driver, we are
less that 100 yards inside the congestion zone which means, that even with my
residents discount, I have to pay just to take my car out of the garage during
the charging hours. But I still think that Whitechapel is a lovely place to
live and it really feels like home to me. There is such a mix of cultures here
and I can meet people from other countries. It feels very comfortable and safe
to me, everything is here and I wouldn’t want to live anywhere else.
Memories of the London Hospital: Summer of 1968
Contributed by Marianne Rapalus Hurley on Dec. 20, 2017
While a nursing student at the University of California Medical Center in San
Francisco, California, I was accepted to a summer work-program at The London
Hospital in Whitechapel. Four women from our nursing class participated, two
at The London Hospital and two at another hospital in the suburbs.
My father worked for United Airlines, so I flew on a stand-by ticket direct
from San Francisco to London. I think it was June since I remember seeing
daffodils. I had no idea how to get from Heathrow Airport to the hospital, so
I took a large black cab that cost a small fortune. The cab delivered me at
the main entrance along Whitechapel Road. I checked in at Matron’s office
where I was assigned a room at Edith Cavell Nurses House, behind the hospital.
Cavell Home, a stately brick building, housed student nurses then and was
named for the World War I heroine, Edith Cavell. Upon entering the building,
there was an office to the left of the foyer. The office contained the one
telephone at Cavell for the nurses’ use. Separating the foyer from the front
office was a counter where a pitcher of milk would sometimes sit (covered with
a folded cloth). Students who wanted milk could help themselves. To the left
of the foyer along a corridor was a reception room to meet visitors. Opposite
the front door was the stairway to the rooms above. I had a private room on
maybe the first or second floor in the rear. It was quite comfortable with a
bed, desk or dressing table, the usual. There were separate bathrooms (aside
from toilet rooms) somewhere in the building; each had a large old-fashioned
tub, great for soaking.
The London Hospital student nurses wore the hospital’s puffy-sleeve (gingham)
uniforms with long skirts, white aprons, and small starched caps. In cooler
weather, the uniform also included a beautiful long cape. At the time, the
students there loved their “old-fashioned” uniform. In fact some were worried
that the National Health or maybe the hospital would modernize it to look more
like my uniform, a plain light blue shirtwaist that resembled something a cafe
waitress might wear. Apparently The London Hospital’s uniforms were updated
sometime after I left. I wonder what the student uniform looks like today. I
wonder if the hospital has its own nursing program any more.
I remember working three days a week in exchange for room and board. I helped
out where needed and ran errands. In 1968 hospital care was simpler with fewer
“gadgets” and far less technology. My first assignment was in Pediatrics; the
“Kids” ward as they called it. Metal cribs with infants and toddlers filled
the large room. I held and rocked many of them during my time there. It was
located I think on an upper floor toward the rear of the main hospital
building and looked out onto the courtyard.
My next assignment was in Men’s Surgical Ward (wish I could remember the exact
name) maybe on the first or ground floor. It was a large ward with 20 or more
beds arranged I think in long rows. I was instructed to make and serve morning
tea on my first day of duty there. I had never done that before, so had to be
taught. A large kettle provided the hot water and I had to remember that the
milk went in first, then the hot tea. I served it to the patients using a
rolling cart. The men were so kind and friendly. I learned that it was the
ward sister who was in charge of not only the patients, but to a large extent,
the doctors too. Sister (named for the ward) was the one who decided when the
dressings and bandages came off. During morning rounds, she participated
completely in the discussions.
Meals for the nurses were in the dining room of the hospital. I think it was
somewhere on the ground floor off the rear courtyard. There was an extensive
buffet to select from. What was new to me was the yellow custard sauce that
was poured on all types of cake and sweets. I came to like it and missed it
when I returned to the states. My friend Kay (the other student nurse from
California) worked in the Accident Department. In pleasant weather we would
meet in the courtyard for lunch. While eating outside, we would often comment
on the residual bomb damage from World War II still visible on the courtyard
walls of the hospital.
The English student nurses would sometimes invite us along for socials on the
weekends. It seemed they used to hang with policemen. At one party we were
driven home by a young policeman who had an old Volkswagen beetle; we fit at
least six nurses in it for the ride home. When a student nurse celebrated a
birthday, we would eat at an Indian restaurant. I may be mistaken, but I seem
to remember we could get a shrimp curry dinner for 11 shillings. (Until that
summer, I had never eaten Indian food). Of course, the money then was the
ancient system of pounds, shillings, and pence; I still miss the old coins
when I visit England.
As part of the program I accompanied a visiting nurse on her rounds in East
London. The nurse wore a uniform suit, maybe navy blue. I remember visiting
mothers and young pre-school children. The families we visited lived in new
high rise buildings that had replaced their older one- and maybe two-story
homes. The mothers complained about the unpleasant elevators, the lack of
private garden space, and the overall drabness of the new buildings. The
visiting nurse was interested in how the neighborhood was changing, so she
shared with me a lot about the history of the East End. What I found
fascinating was the physical evidence of that history still there in 1968.
There were still so many brick residences along narrow streets, the waterfront
pubs, and simple shops, 19th century buildings that were slowly being
replaced. In general Whitechapel did not draw tourists then, (there were no
‘Jack the Ripper’ tours), but there were many historic areas “off the beaten
path” to explore.
The last time I visited The London Hospital, (well, now the Royal London)
about eight or ten years ago, I could not find Cavell Home. They were
constructing a very tall bright blue high rise (incompatible architecturally)
behind the old hospital. Things looked very different and I became
disoriented. It was disturbing and sad to see the loss of the hospital complex
that I had experienced long ago. I assume the old London buildings along
Whitechapel Road are now abandoned on the interior; online photos show the
wards, surgeries, and offices empty. I wonder what they are planning now.
Yes, I wish I had taken more photographs during that time, especially in light
of the drastic recent changes. With its human-scale Georgian brick buildings,
The London Hospital in 1968 felt like a unique combination of stepping back in
time while participating in modern medical care. I treasure my memories and
very grateful for that experience nearly 50 years ago.
Bad memories of the London
Contributed by patricia on July 5, 2017
I used to hate to go to the London Hospital (when did it become The Royal
London?) if we had to visit a sick relative. Plus any of my relatives who went
in didn't come out. It always smelled of antiseptic and food and the uniforms
the nurses wore looked so old fashioned to me (a young, modern girl) as
opposed to the modern uniforms you would see on hospital shows on the telly.
My father died in 1954 when I was 5 and was taken to the London, but they
couldn't save him from a massive heart attack. He was only 35. The London had
bad memories for me. Plus I had an accident at school when I was about 8 or 9,
at Robert Montefiore Primary on Deal Street, opposite where I lived. I was
running up the stairs with a tray of glass jars they used for painting, fell
over and cut my hand on one of the broken jars. They called an ambulance and
took me to the London, where they gave me a few stitches in my hand. An awful
memory for a young child. My auntie Ann lived in a street behind the hospital,
Nelson Street, and I hated walking past the place when we went to visit her.
Memories of Priscilla Church
Contributed by Shahed Saleem on Aug. 31, 2016
Priscilla Church was a student nurse at the Royal London Hospital from 1982 to
1985, and a staff nurse until 1986. She then returned to the hospital as a
midwife from 1993-1996. These are some of her recollections of her time there:
The flats [Knutsford House] were really nice – a tiny kitchen and bathroom, a
living room and bedroom. I was very comfy for the year I lived there when I
was working as a midwifery sister, in the 1990s. I looked out at the front and
the helicopter landed just outside which was really interesting especially as
it was quite a new ‘ambulance’.
The other homes I lived in as a student nurse were initially Mildmay Mission
hospital in Shoreditch (now an HIV/Aids hospice); Luckes; Cavell; John
Harrison and Brierley. The last two were in Philpott Street.
We never discussed the uniform either. When I started as a student nurse the
hospital had a uniform room where seamstresses made the uniforms to measure.
We had detachable collars so that you would change your collar and apron each
shift and the dress a couple of times a week. We had removal buttons as well
as a collar stud which all had to be removed for laundering, which was done at
the hospital too. We also had a starched cap which took some time to make up.
Aprons were starched white cotton and only ever worn on the ward. Any duties
that took you off the ward e.g. going to pharmacy, one took the apron off. I
always get very annoyed in films, or tv where a nurse will where an apron when
not on the ward. We had lovely purple cloaks for travelling between the nurses
home and the ward. They were also useful on night duty during our breaks –
they made a good blanket to keep us warm – four o’clock in the morning is a
very cold time. The students wore purple gingham; staff nurses were in purple
and sisters wore blue and had detachable sleeves and frills on their caps.
‘Purple passions’ were ill-fitting uniforms worn by students in their first
eight weeks when we might visit a ward for a few hours. This was during our
induction when we were based in the school of nursing (Philpott Street) (and
before our made to measure uniforms were ready). Although modern uniforms are
easier to wear and launder I always felt that we looked very smart and
professional in the old uniform. One of the seamstresses in the uniform room
was willing to make a copy of the student uniform for a ‘big doll’; which I
had made and still have and love.
Birthplace
Contributed by steve on Nov. 5, 2016
I made my way into the world in the Marie Celeste Ward of the London Hospital
in December 1949. I have many memories of visits to this hospital for broken
arms, a stiff neck and other forms of accidents etc. A lasting memory, which
although at the time did not mean much to me, was being asked by my headmaster
Rhodes Boyson to deliver a letter to a Professor Francis Camps.
Like others who lived in the East End, this hospital holds many memories, some
good, some not quite so good but again like many others, we owe so much to
this place and the marvelous staff who, throughout the years, have worked
within its walls.
The Jewish community
Contributed by Jil on June 13, 2017
The small terraced houses behind the London Hospital were occupied by local
residents for much of the time I worked there in the 1960s. Previously I had
very little contact with the strict Jewish community, apart from the
occasional Liberal Jewish patient in the hospital in Brighton, where I had
trained as a nurse. One day, on my way back to John Harrison House, the new
nurses' home, in uniform, having just come off duty, I was called out to by an
elderly woman at her front door asking if I could help her. When I went to her
door, she asked me if I could come in and light her fire. Surprised at this
request, I went in to find the fire already laid and it just needed a match
put to it. I lit the fire and then asked her why she had not been able to do
this herself. She gently explained that it was past dusk on Friday evening,
her Sabbath, and her religion prevented her from doing any work, including
lighting the fire. My first, but not my last, experience of the strict Jewish
community in the area at that time. From then on, each week, when I could, I
called into the same woman to light her fire and have the occasional cup of
tea with her; which I made and drank without milk. To this day, I still drink
tea without milk!